A
MEDLEY
OF
PRACTICE APPROACHES
Social Work Assessment:
Case Theory Construction
by Cynthia
D.
Bisman
Abstract
To
intervene effectively, social workers need to make sense
of
clients and their situations.
A
case theory approach to assessment pro-
vides a framework to
formulate
assessments that are clear and directly
related
to the real-world problems clients present Explaining
the problem situation,
case
theory
forms
the foundation for
selection
of
intervention
strategies
and methods to achieve change. Build-
ing case theory requires practitioner abilities to
form
concepts,
relate
concepts
into
propositions,
develop hypotheses, and organize
these into a coherent whole. Including
case
background information,
observations
and relevant professional literature,
case
theory pre-
sents an accurate and cogent comprehension
of
the client
Two
case
examples
of
depression illustrate the important relationship
among concepts, empirical referents, propositions, general theorles, and intervention, highlighting how case theory guides practice.
AN OVERARCHING INQUIRY DIRECTS this article:
How do social workers figure out what is going
on
with
clients? Embedded within is another question: What is
the point of this knowledge?
I
offer here a case theory
framework for use by social workers to make sense
of
cli-
ents and their situations and connect that comprehension
to treatment planning and intervention.
In social work, it is the assessment that determines
the nature of the client’s current situation at a particular
point in time. Resulting in the product
of
a written as-
sessment (variously called a psychosocial study, intake re-
port, or social history, among other nomenclature) and
entailing specific tasks such as observing and interview-
ing clients along with data gathering, the process of as-
sessing is often ignored. Yet, without a clear framework
for thinking about and engaging in the process of assess-
ment, the products will be flawed and either useless to
the social worker, or harmful to the client, or both.
Through gathering data that determines the relevant
attributes of each case, social work assessment provides
the “here and now” and how
it
got that way. A far more
complex and significant process than data collection, as-
sessment also incorporates the tasks of deciding which
data to seek and how to organize it. Moreover, all prac-
tice components flow from the assessment that shapes
the character of the professional relationship, impacts
on
communication methods and skills, directs social work
intervention, determines measurements and data collec-
tion needs, and guides evaluation. As a joint activity by
both the social worker and the client, assessment requires
their mutual understanding and agreement. Engaged in a
journey together, social workers and clients work
to
de-
termine the nature
of
the problem causing the client dif-
ficulty
so
that they can change the situation.
Assessment was an effort by Mary Richmond to
make the social work profession more scientific.
In
her
Social
Diagnosis
(1917), she provides a lengthy and de-
tailed method for obtaining social evidence, which was
used by the social worker for understanding the client’s
difficulties and deciding “what course
of
procedure” to
follow (p. 39). She states, “social diagnosis is the attempt
to arrive at as exact a definition as possible
of
the social
situation and personality
of
a given client. The gathering
of evidence, or investigation, begins the process, the crit-
ical examination and comparison
of
evidence follows,
and last come its interpretation and the definition of the
social difficulty” (p.
62).
Social work has not yet reached a consensus on the
structure and function of assessment. Some in the profes-
sion criticize a current trend
to
substitute psychodiagno-
sis for social work assessment by relying
on
prepackaged
scales such as the
DSM-IV
(Mattaini
&
Kirk, 1993; Ab-
bott, 1988; Ikver
&
Sze, 1987). Others, like Hudson
(1990),
call for heavy reliance
on
computers and stan-
Families in Society: The Journal
of
Contemporary Human Services
Copyright
1999
Families International, Inc.
240

Bisman Case
Theory
Construction
dardized scales, and Hopton (1998) reports on the use of
psychological profiles in risk assessments.
Importance
of
a Case
Theory
Approach
to
Assessment
For social work assessments that are clear and directly
related to the real-world problems that clients present, case
theory provides a means
of
conceptualizing assessment and
formulating assessments that are not only accurate and in-
formative but also lead directly
to
relevant interventions.
Case theory provides a set
of
ideas to understand and treat
the symptoms or problems in functioning of one particular
client (client may refer to an individual, family, group, com-
munity, or organization).
Consider the following situation facing Melissa, a social
worker employed for
two
years by a child guidance center.
The eight-year-old client, Edith, is in second
grade and has been residing with her maternal
grandmother for the past year along with her
ten-year-old sister and two older male cousins.
Edith cries often, is uncommunicative at home,
picks fights with children at school, and does
poorly in school work. Records show that
Edith’s mother abused drugs and had several
abusive relationships. Edith does not know her
father, who is incarcerated.
How does Melissa understand these facts? She looks
closely at Edith’s sad face and remembers information
from her classes about attachment theory (Bowlby, 1977)
that discontinuities of parenting can result in depression.
Melissa has always been drawn to object relations theo-
ry (Winnicott, 1989), which offers her a way of under-
standing Edith’s problems. Melissa decides that Edith has
poor social relations with others because her split be-
tween good and bad was not resolved before she reached
one year old and because of that she has low self-esteem
resulting from lack of a supportive caregiver during in-
fancy. Deciding that Edith is depressed, Melissa recom-
mends weekly therapy sessions to help increase her self-
esteem, utilizing play and supportive group therapy.
What
do
we think of Melissa’s approach to this case
and how she came to an understanding about Edith?
Some may worry that Melissa was too quick with her di-
agnosis
of
depression, possibly neglecting other explana-
tions for Edith’s problematic behaviors. What
if,
instead
of struggling with issues in her past, Edith is being
abused now, possibly
by
her older male cousins? Or per-
haps her symptoms are the result of her mother’s drug
use during pregnancy? Most of us can probably agree
that Melissa needs a fuller understanding to be sure she
is
on
the right track. More information is necessary
about Edith’s current home environment along with a
learning assessment from the school and a current medi-
cal examination. If Edith is currently residing in an abu-
sive situation, she continues
to
be at risk without inter-
vention aimed at providing her with a safe environment.
Likewise, should Edith have physiological problems
making learning difficult for her, targeted help from the
school at this early age could prove highly productive.
Missing in Melissa’s assessment and intervention is a
deliberative process of building an understanding that ac-
curately explains her client’s symptoms.
A
case theory
approach to assessment provides a structure for social
workers to follow in comprehending their clients. This
framework emphasizes utilization of relevant contempo-
rary literature and direct focus
on
the empirical evidence
in
the client’s life. Conceptualizing assessment as case
theory building enables practitioners to articulate what is
happening with a particular client at one specific point in
time and is essential to an intervention that is germane to
that client and relevant to the presenting problem and
context of the client situation.
Building case theory demands the knowledge about
concepts and theory construction and the skills
to
relate
concepts into propositions, develop hypotheses, and
avoid deductive and inductive fallacies. Let us review
these terms and then illustrate their use in formulating a
case theory.
Theory
As
Bisman and Hardcastle (1999) explain, pursuit of
theory
is
to provide orderly explanations of the confu-
sions in life experiences. In drawing patterns from obser-
vations to explain phenomena, different persons may ex-
plain the same events with a range
of
theories. The theory
is not real but rather is the individual’s attempt to explain
real things. They further emphasize that available tech-
nologies and contemporary ideologies influence theories
by discussing the contrast in theories about depression
from the 1970s with those in the 1990s. Freudianism
dominated the 1970s explaining depression
as
a primar-
ily psychological phenomenon. In the 1990s pharmacol-
ogy is the mode, viewing depression as a bio-chemical
imbalance while gene research offers new ways
to
under-
stand and explain the etiology
of
what was once consid-
ered solely a “mental” disorder. They predict more rapid

FAMILIES
IN
SOCIETY
May
-
June
7999
T&?
idea:
Labt.l:
The
IIlentdl
The
word
or
picture
and words represent-
Lonwwmm
ot
ing
the
idea.
\\
orld.
\otllt‘
pdrt
ot
[he
shifts with increasing advances in technological knowl-
edge.’
Constructions by individuals to order events, theories
offer logical conclusions based on presented relationships.
Other than final proofs of logic and mathematics, which
stem from stated premises and are not from or about the
empirical world, theories do not offer universal laws bur
rather present different levels
of
abstractness (some, such
as Lakoff and Nunez, 1997, believe that even abstract
mathematical concepts are based on human experience).
Perhaps one
of
the more elegant definitions of theo-
ries is offered by Karl Popper (1982) when he refers to
“theories as human inventions
-
nets designed by
us
to
catch the world” (p.
42),
warning that “there is no ahso-
lute measure for the degree
of
approximation achieved
-
for the coarseness or fineness of the net”
(p.
47).
Whether grand, scientific, or case, theory
is
a sys-
tematically related set
of
propositions that explain and/or
predict phenomena (Dubin, 1978,
pp.
15-32; Lewis,
1982, pp. 18,
61-63;
Reynolds, 1971,
pp.
10-11,
87-
1
14).
While theories are not inherently “real” or “hypo-
thetical,” their usefulness as constructions increase the
more they can explain and predict. Theories range
through levels
of
abstractness from grand theories that
explain a lot
of
phenomenon
to
very concrete and cir-
cumstantial case theories that are locked in a specific
time, place, and event. Freudian theory offers explana-
tion
of
all human development and behavior and
is
an
example of a grand theory. Good case theory provides
understanding
of
the case, explaining why a particular
client is behaving in a certain manner, laying the foundci-
tion for prediction of interventions necessary
to
accom-
plish the case objectives and case change.
%e
&h€:
The thing
in
the
world
captured
by
the idea.
Concept Formation
Case theory building requires specification and de-
velopment
of
concepts
-
the fundamental units and
building blocks
of
propositions and theories. For practi-
tioners
to
understand the meaning
ot
case theory, they
must understand the theory’s concepts. Ideas in the
mind.
concepts are the words or labels symbolizing the external
things that the ideas represent. Just as we discussed with
theories, concepts are not reality but represent a mental
construction
of
realit!..’
The mental and empirical processes of developing
and operationalizing concepts and relating the concepts
to
explain and predict things is theory building. I’racti-
tioners must relate concepts in case theory to each other.
It
the case theory building is faulty, interventions based
on
the theory are not likely
to
produce the intended re-
sults and may result in harm.
I
Jnderstanding
concept
starts with three components
illustrated in Table
1
below:
I.
The idea or mental image and construction in the
2.
The words or labels symbolizing the idea, and
3.
The external thing, phenomena, and empirical refer-
ents in the world represented by the labels.
mind.
Table
1.
I
Child abuse
1
I
!
Conceptualization is the process
of
assigning words
to ideas, abstractions, and constructions
of
empirical re-
slit!-
that have empirical references. Practitioners must
not reify the concept by assuming that the idea is real or
the only construction
of
reality. It is also important
to
de-
\,rlop the nominal detinition and domain
of
the concept
tu
distinguish empirical referents that fall within the idea
trom those that do not. Operational definitions that cap-
rurc the idea are prerequisite
to
concepts that are usable
in
c~se theory.
Propositions and Hypotheses
Theories are composed
of
propositions,
which are
statements about the relationships among elements, con-
cepts, or attributes
of
one or more concepts. Propositions
allow
us
to understand concepts and relate and integrate
them into theory. The task in building and reviewing the-
ory. including case theory,
is
to
find the “if-then’’ propo-
<itions that constitute the theorv to explain the case and
provide prediction
for
the appropriate intervention.
Hypotheses
are propositions that are capable of em-
pirical testing but as yet are untested. One function
of
re-
Fearch is to test and establish the validity of hypothetical
propositions. Deduced from theorv or induced from em-
‘
The
following
sections
ovi
theory draw
from
Bismm and
Wilrdc-astle,
1999.
chapter
four.
‘Blumer’s
(1
969)
iiwk
OIZ
symbolic interactionism influences
thesc
ideas.
Bisman Case Theory Construction
pirical generalizations and experiences, their purpose is to
extend the explanatory and/or predictive capacity of theo-
ry or to explain empirical generalizations and experiences.
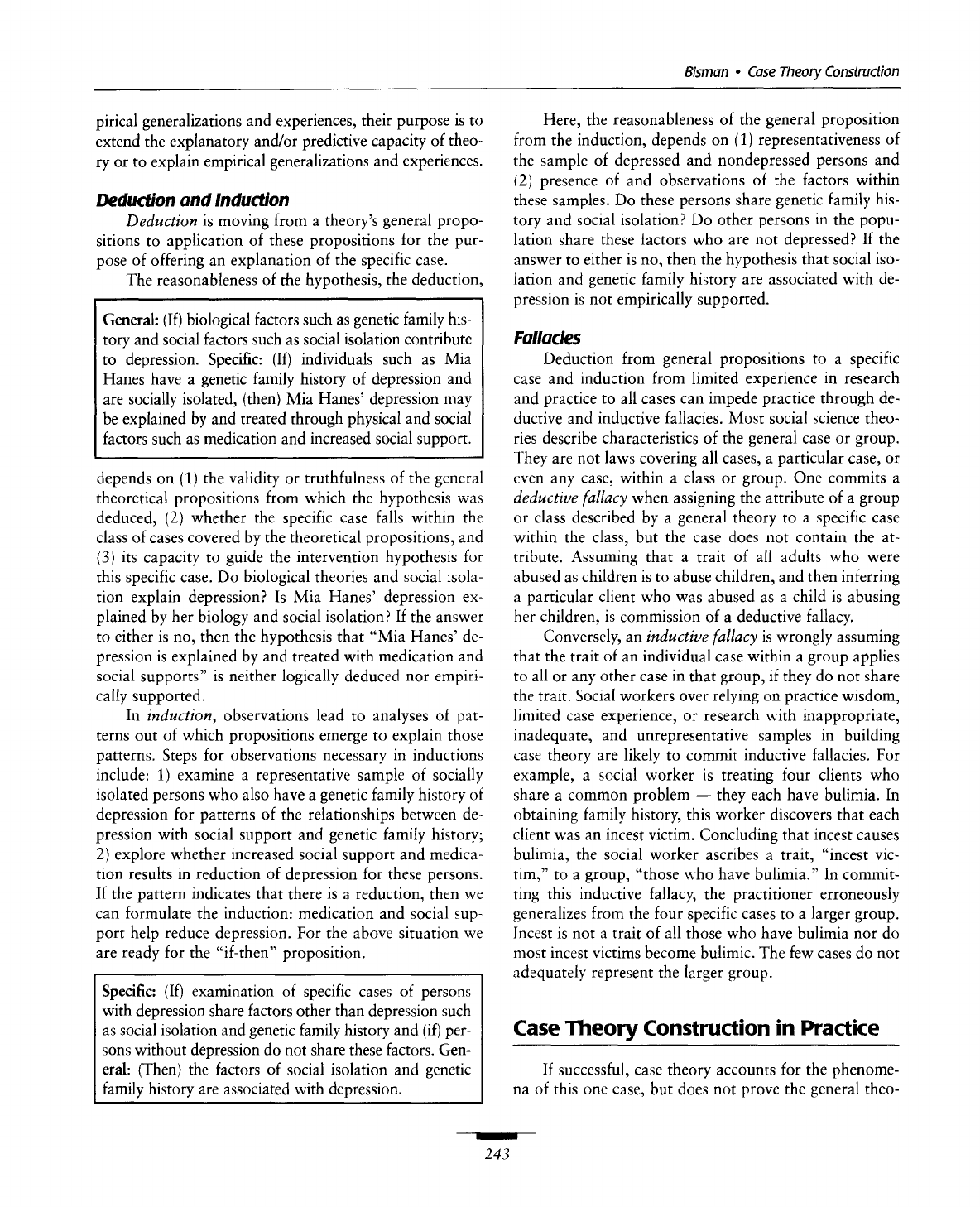
Deduction and Induction
Deduction
is moving from a theory’s general propo-
sitions to application of these propositions for the pur-
pose of offering an explanation of the specific case.
The reasonableness of the hypothesis, the deduction,
General: (If) biological factors such as genetic family his-
tory and social factors such as social isolation contribute
to depression. Specific: (If) individuals such as Mia
Hanes have a genetic family history of depression and
are socially isolated, (then) Mia Hanes’ depression may
be explained by and treated through physical and social
factors such as medication and increased social support.
depends on
(1)
the validity or truthfulness of the general
theoretical propositions from which the hypothesis was
deduced,
(2)
whether the specific case falls within the
class
of
cases covered by the theoretical propositions, and
(3)
its capacity to guide the intervention hypothesis for
this specific case.
Do
biological theories and social isola-
tion explain depression?
Is
Mia Hanes’ depression ex-
plained by her biology and social isolation? If the answer
to either is no, then the hypothesis that “Mia Hanes’ de-
pression is explained by and treated with medication and
social supports” is neither logically deduced nor empiri-
cally supported.
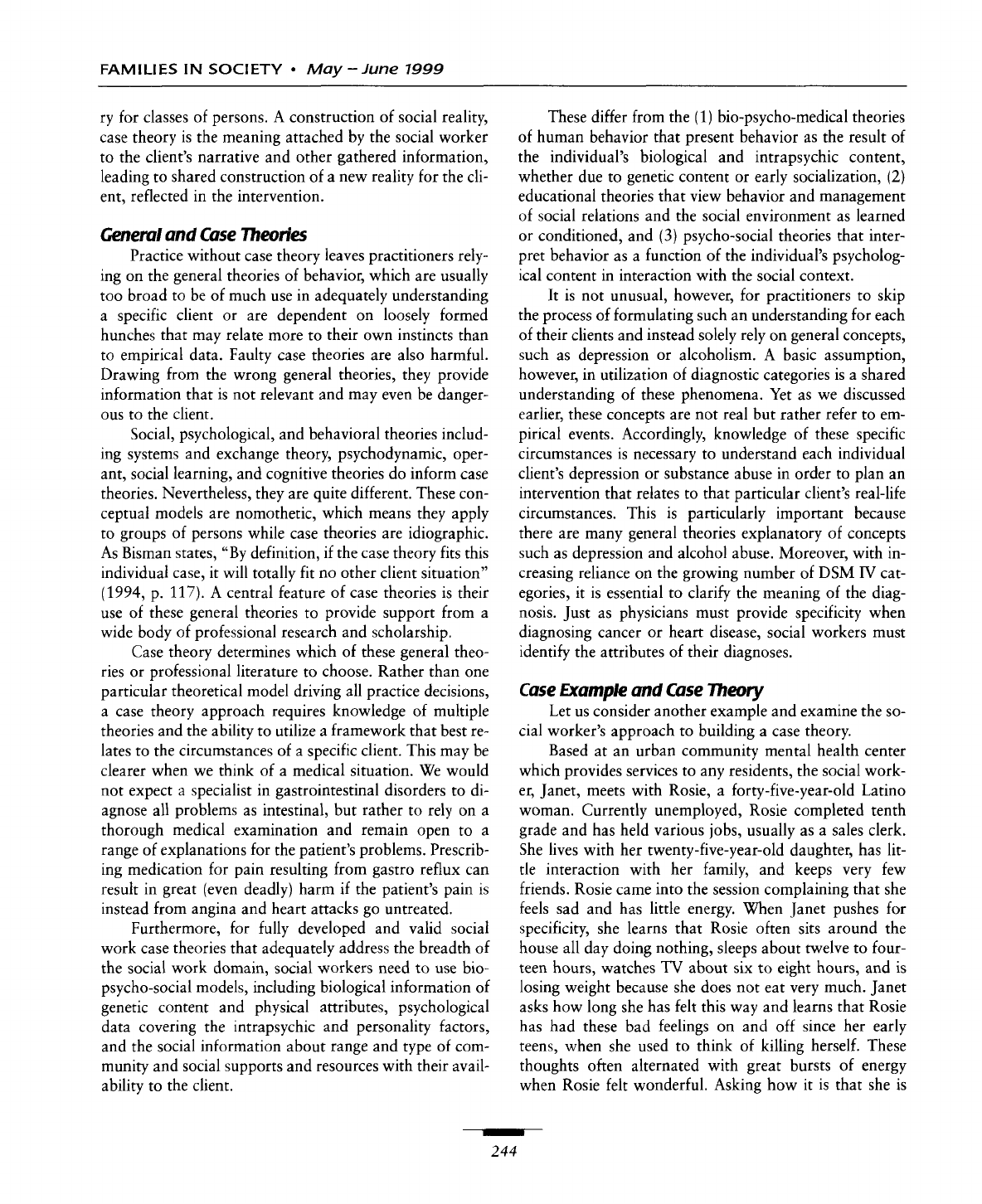
In
induction,
observations lead to analyses of pat-
terns out of which propositions emerge to explain those
patterns. Steps for observations necessary in inductions
include:
1)
examine a representative sample of socially
isolated persons who also have a genetic family history of
depression for patterns of the relationships between de-
pression with social support and genetic family history;
2)
explore whether increased social support and medica-
tion results in reduction of depression for these persons.
If the pattern indicates that there is a reduction, then we
can formulate the induction: medication and social sup-
port help reduce depression. For the above situation we
are ready for the “if-then’’ proposition.
Specific: (If) examination of specific cases of persons
with depression share factors other than depression such
as social isolation and genetic family history and
(if)
per-
sons without depression do not share these factors. Gen-
eral: (Then) the factors of social isolation and genetic
family history are associated with depression.
Here, the reasonableness
of
the general proposition
from the induction, depends on
(1)
representativeness of
the sample
of
depressed and nondepressed persons and
(2)
presence of and observations of the factors within
these samples. Do these persons share genetic family his-
tory and social isolation?
Do
other persons in the popu-
lation share these factors who are not depressed? If the
answer to either is no, then the hypothesis that social iso-
lation and genetic family history are associated with de-
pression is not empirically supported.
Fallacies
Deduction from general propositions to a specific
case and induction from limited experience in research
and practice to all cases can impede practice through de-
ductive and inductive fallacies. Most social science theo-
ries describe characteristics of the general case or group.
They are not laws covering all cases, a particular case, or
even any case, within a class or group. One commits a
deductive
fallacy
when assigning the attribute of a group
or class described by a general theory to a specific case
within the class, but the case does not contain the at-
tribute. Assuming that a trait of all adults who were
abused as children is to abuse children, and then inferring
a particular client who was abused as a child is abusing
her children, is commission of a deductive fallacy.
Conversely, an
inductive
fallacy
is wrongly assuming
that the trait of an individual case within a group applies
to all or any other case in that group,
if
they do not share
the trait. Social workers over relying on practice wisdom,
limited case experience, or research with inappropriate,
inadequate, and unrepresentative samples in building
case theory are likely to commit inductive fallacies.
For
example, a social worker is treating four clients who
share a common problem
-
they each have bulimia. In
obtaining family history, this worker discovers that each
client was an incest victim. Concluding that incest causes
bulimia, the social worker ascribes a trait, “incest vic-
tim,” to a group, “those who have bulimia.” In commit-
ting this inductive fallacy, the practitioner erroneously
generalizes from the four specific cases
to
a larger group.
Incest is not a trait of all those who have bulimia nor do
most incest victims become bulimic. The few cases do not
adequately represent the larger group.
Case
Theory
Construction in Practice
If
successful, case theory accounts for the phenome-
na of this one case, but does not prove the general theo-
I
243
FAMILIES
IN
SOCIETY
May
-
June
7999
ry for classes of persons. A construction of social reality,
case theory is the meaning attached by the social worker
to
the client’s narrative and other gathered information,
leading to shared construction
of
a new reality for the cli-
ent, reflected in the intervention.
General and Case
Theories
Practice without case theory leaves practitioners rely-
ing
on
the general theories of behavior, which are usually
too broad to be of much use in adequately understanding
a specific client
or
are dependent
on
loosely formed
hunches that may relate more to their own instincts than
to empirical data. Faulty case theories are also harmful.
Drawing from the wrong general theories, they provide
information that is not relevant and may even be danger-
ous
to the client.
Social, psychological, and behavioral theories includ-
ing systems and exchange theory, psychodynamic, oper-
ant, social learning, and cognitive theories do inform case
theories. Nevertheless, they are quite different. These con-
ceptual models are nomothetic, which means they apply
to groups
of
persons while case theories are idiographic.
As Bisman states,
“By
definition,
if
the case theory fits this
individual case,
it
will
totally
fit
no
other client situation”
(1994,
p.
117).
A central feature of case theories is their
use of these general theories to provide support from a
wide body of professional research and scholarship.
Case theory determines which
of
these general theo-
ries or professional literature to choose. Rather than one
particular theoretical model driving all practice decisions,
a case theory approach requires knowledge
of
multiple
theories and the ability to utilize a framework that best re-
lates to the circumstances
of
a specific client. This may be
clearer when we think of a medical situation. We would
not expect a specialist in gastrointestinal disorders
to
di-
agnose all problems as intestinal, but rather to rely
on
a
thorough medical examination and remain open to a
range
of
explanations for the patient’s problems. Prescrib-
ing medication for pain resulting from gastro reflux can
result in great (even deadly) harm if the patient’s pain is
instead from angina and heart attacks
go
untreated.
Furthermore, for fully developed and valid social
work case theories that adequately address the breadth
of
the social work domain, social workers need
to
use
bio-
psycho-social models, including biological information of
genetic content and physical attributes, psychological
data covering the intrapsychic and personality factors,
and the social information about range and type of com-
munity and social supports and resources with their avail-
ability to the client.
These differ from the
(1)
bio-psycho-medical theories
of human behavior that present behavior as the result of
the individual’s biological and intrapsychic content,
whether due to genetic content or early socialization,
(2)
educational theories that view behavior and management
of social relations and the social environment as learned
or conditioned, and
(3)
psycho-social theories that inter-
pret behavior as a function
of
the individual’s psycholog-
ical content in interaction with the social context.
It is not unusual, however, for practitioners to skip
the process of formulating such an understanding for each
of their clients and instead solely rely
on
general concepts,
such as depression or alcoholism. A basic assumption,
however, in utilization of diagnostic categories is a shared
understanding of these phenomena. Yet as we discussed
earlier, these concepts are not real but rather refer to em-
pirical events. Accordingly, knowledge of these specific
circumstances is necessary
to
understand each individual
client’s depression or substance abuse in order
to
plan an
intervention that relates to that particular client’s real-life
circumstances. This is particularly important because
there are many general theories explanatory
of
concepts
such as depression and alcohol abuse. Moreover, with in-
creasing reliance on the growing number of DSM
IV
cat-
egories,
it
is essential to clarify the meaning
of
the diag-
nosis. Just as physicians must provide specificity when
diagnosing cancer or heart disease, social workers must
identify the attributes of their diagnoses.
Case Example
and
Case
Theory
Let
us
consider another example and examine the
so-
cial worker’s approach
to
building a case theory.
Based at an urban community mental health center
which provides services
to
any residents, the social work-
er, Janet, meets with Rosie, a forty-five-year-old Latino
woman. Currently unemployed, Rosie completed tenth
grade and has held various jobs, usually as a sales clerk.
She lives with her twenty-five-year-old daughter, has lit-
tle interaction with her family, and keeps very few
friends. Rosie came into the session complaining that she
feels sad and has little energy. When Janet pushes for
specificity, she learns that Rosie often sits around the
house all day doing nothing, sleeps about twelve to four-
teen hours, watches
TV
about six
to
eight hours, and
is
losing weight because she does not eat very much. Janet
asks how
long
she has felt this way and learns that Rosie
has had these bad feelings
on
and off since her early
teens, when she used
to
think
of
killing herself. These
thoughts often alternated with great bursts of energy
when Rosie felt wonderful. Asking how it is that she is
I
244

Bisman
Case
Theory
Construction
now asking for help, she learns Rosie feels worse since
testing positive for
HIV,
three months ago.
Janet formulates the following case theory:
Rosie’s recent
HIV
diagnosis is exacerbating
her
long
term social isolation and possible clini-
cal depression. Goldstein (1995) and Jue
(1
994), indicate that stigma from
AIDS
often
socially isolates these patients, while Mancoske
(1
996) points to their greater risk of suicide.
In-
dividuals need an active energy exchange with
others as Greene
(1
991) explains in her discus-
sion of systems theory, and for a long time Rosie
has had
no
person with whom she can talk
openly. Her long history of severe
mood
swings
suggests bipolar disorder. Evidence supports a
biological basis
for
treatment of depression
(Sperry, 199.5). Jensen
(1
994) points to
a
psy-
chosocial perspective combined with
a
biologi-
cal perspective.
Because she knows we can use the concept
of
depres-
sion
to
describe different conditions, Janet identifies the
empirical indicators relevant for each client labeled as de-
pressed. The empirical behaviors for Rosie include the
following problems: sleeps an average
of
thirteen hours
per day, shows a decrease in appetite, has severe mood
swings, and an overall lack of functioning with extensive
Developed from data collection and
observations, case theory presents social
workers’ understanding
of
a particular
client‘s problematic condition at a
specific point
in
time.
periods of sitting around and watching television.
Propositions in Janet’s case theory pose a
relationship between social isolation, illness, biology, and
depression. Janet’s hypothesis is a deduction that Rosie’s
symptoms are explained by her biology, social isolation,
and disease. Correspondingly, Janet refers to general the-
ories of systems, biological and psychological, and social
explanations for understanding depression and the psy-
chosocial effects of
AIDS.
Emerging from this case theory, Janet’s intervention in-
cludes both increasing social supports and a medical con-
sult to consider pharmacology for the possible bipolar
disorder. Focus on just AIDS, or only the social isolation,
or solely the clinical depression ignores important vari-
ables. Janet is aware that any of these narrow interven-
tions is potentially harmful to Rosie.
When we compare Janet’s approach to understand-
ing Rosie with our earlier example of Melissa, we can see
the enhanced practice by Janet who is able to directly link
this understanding to her intervention based on concrete
evidence. The clear statement of her case theory’s propo-
sitions and hypotheses and identification of the general
theories she uses prevent fallacies in her thinking.
By
broadly basing her case theory to incorporate multiple
hypotheses, she logically draws from a range
of
general
theories resulting in a plan of intervention that addresses
the breadth of social work practice by including biologi-
cal,
psychological, and social factors.
Summary
In response to the initial questions of how social
workers make sense of clients and what they do with that
information, we have examined a case theory approach
to social work assessment requiring comprehension of
theory, specification of concepts, and development of
propositions and hypotheses. Emphasis is on the linkages
between building a theory of the case with accurate client
assessments and relevant subsequent practice interven-
tions. While recognizing the importance
of
case theory
constructions
by
practitioners, this framework also dis-
tinguishes case theory from those general theories found
in the literature.
Case theory, like all theory, is explanation of phe-
nomena. Idiographic, case theory applies only to a spe-
cific case and is distinct from social and behavioral theo-
ries, which are nomothetic and apply generally to groups
of persons. Developed from data collection and observa-
tions, case theory presents social workers’ understanding
of a particular client’s problematic condition at a specif-
ic point in time.
As
Florence Hollis
(1970)
stressed in her
development of the psychosocial approach, the purpose
of assessment is to develop the basis for treating each cli-
ent as a separate individual. Addressing specific empirical
events, the test
of
the case theory is the extent to which
it
explains this unique client, accounts for the phenomena,
and guides a successful intervention. Case theory con-
nects this client’s past to the present and future in order
I
245

FAMILIES
IN
SOCIETY
May-June
7999
to project a future set of events
-
the change in the cli-
ent’s presenting problems (Bisman,
1994).
Social workers must consider and confront both
social context and individual content of behavior and ac-
cordingly rely
on
bio-psycho-social theories where
behavior is a function
of
the individual client’s biological
and psychological content and the social context
-
the
social work domain.
Social work practice involves using and testing theo-
ries.
To
formulate their assessments, social work practi-
tioners require theory-building knowledge and skills.
Building case theory requires practitioner abilities to
form concepts, relate concepts into propositions, develop
hypotheses, and organize these into
a
coherent whole.
From case theory’s coherent explanation
of
the empirical
referents and reference to general theories and wide pro-
fessional knowledge, come selection of intervention
strategies with methods to change the presenting prob-
lems. Including client background information and perti-
nent professional literature, case theory presents a cogent
and valid comprehension of the client, a prerequisite for
appropriate interventions that are helpful to clients.
Jensen,
C.
(1994). Psychosocial treatment
of
depression in women:
Nine single-subject evaluations.
Research
on
Social Work Prac-
tice,
4,
267-282.
Jue,
S.
(1994). Psychosocial issues
of
AIDS
long-term survivors.
Fami-
lies in Society,
75(6), 324-332.
Lakoff,
G.,
&
Nunez, R. (1997).
In
L. English (Ed.),
Mathematical rea-
soning: Analogies, metaphors, and images.
Erlbaum.
Lewis,
H.
(1982).
The intellectual base
of
social work practice.
New
York: Haworth Press.
Mancoske,
R.
(1996). HIV/AIDS and suicide: Further precautions.
So-
cial Work,
3,
325-326.
Mattaini,
M.,
&
Kirk,
S.
A. (1993), Points and viewpoints: Misdiag-
nosing assessment.
Social Work,
38,231-233.
Popper,
K.
(1982). The open universe: An argument
for
indeterminism.
(From the postscript to
The Logic
of
Scientific Discovery,
origi-
nally published as
Logik der Forschung
in 1935 and revised,
1959). Totowa,
NJ:
Rowman
&
Littlefield.
Reynolds,
P.
(1971).
A
primer
in
theory construction.
New York:
Macmillan.
Richmond,
M.
(1917).
Social diagnosis.
New York: Russell Sage Foun-
dation.
Sperry, L. (1995).
Psychopharmacology and psychotherapy: Strategies
for maximum treatment outcomes.
New York: Bruner Mazel.
Winnicott, D.
W.
(1989).
Psychoanalytic explorations.
Cambridge,
MA:
Harvard University Press.
References
Cynthia
D.
Bisman
is
associate
professor,
Bryn
Mawr College, Graduate
School of Social
Work
Bryn
Mawr,
PA.
Abbott,
A.
(1988).
The system of professions: An essay
on
the division
of
expert labor.
Chicago: University
of
Chicago Press.
Bisman, C. D. (1994).
Social work practice: Cases and principles.
Pa-
cific Grove, CA: BrookslCole.
Bisman,
C.,
&
Hardcastle, D. (1999).
Integratrng research into prac-
tice:
A
model
for effective social work.
Pacific Grove,
C,4:
Brooks/Cole.
Blumer,
H.
(1969).
Symbolic interactionism.
Englewood Cliffs, NJ:
Prentice-Hall.
Bowlby,
J.
(1977). The making and breaking of affectional bonds.
British journal of Psychiatry,
230,
201-10.
Dubin,
R.
(1978).
Theory building.
New York: Free Press.
Goldstein,
E.
G. (1 995). Working with persons with AIDS. In E. Gold-
man (Ed.),
Ego
psychology and social work practice
(pp. 274-
281). New York: Free Press.
Greene, R.
R.
(1991). General systems theory.
In
R.R. Greene
&
P.
H.
Ehross (Eds.),
Human behavior and social work practice,
(pp.
227-259). New York: Aldine De Gruyter.
Hollis,
F.
(1970). The psychosocial approach tn the practice of case-
work.
In
R. Roberts
&
R. Nee (Eds.),
Theories of social casework,
(pp. 33-76). Chicago: University
of
Chicago Press.
Hopton,
J.
(1998). Risk assessment using psychological profiles tech-
niques: An evaluation of possibilities.
The British Journal nf
So-
cial Work,
28(2), 247-261.
Hudson,
W. W.
(1990). Computer based clinical practice.
In
L.
Videka-
Sherman
&
W.
J.
Reid (Eds.),
Advances
in
clinical social work
re-
search
(pp.
105.117).
Silver Spring,
MD:
NASW
Press.
Ikver, B.,
&
Sze, W. (1987). Social work and the psychiatric nosology
of schizophrenia.
Social Casework,
68,
131-139.
Author’s note: The author acknowledges thefollowing
Bryn
Mawr
MSS
studentsfor their case material: Jacqueline Stahl
and
Janine Wettrtone.
Original manuscript received:
July
1, 1998
Revision received December
28,
1998
Accepted: January 1, 1999
I
246
